
Residential Segregation and Health: A Hypothesis Still in Search of Convincing Evidence
As Arcaya and Schnake-Mahl note in their article “Health in the Segregated City”, race or ethnicity and poverty are strongly associated with health. Table 1 demonstrates this well-known fact with data drawn from the 2010 to 2016 National Health Interview Surveys (NHIS).
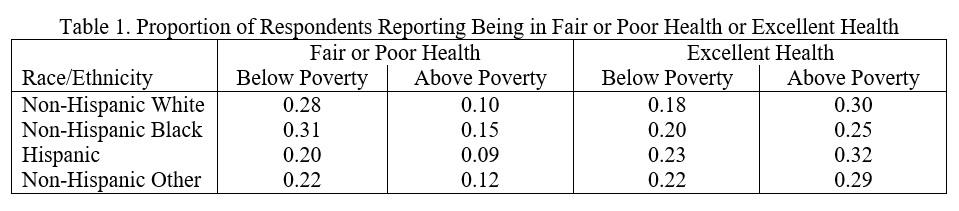
The figures in Table 1 are unsurprising. Being poor is strongly associated with worse self-reported health, and this is true for all racial or ethnic groups. The race/ethnicity-specific differences in health between poor and non-poor are largest for White persons. Race/ethnicity is also associated with self-reported health (within poverty group). Notably, within each poverty group, differences between White and Black persons are small compared to differences between poverty groups within race. It is also evident that Hispanic persons and those labeled as Other (race) have the best health among the four race/ethnic groups.
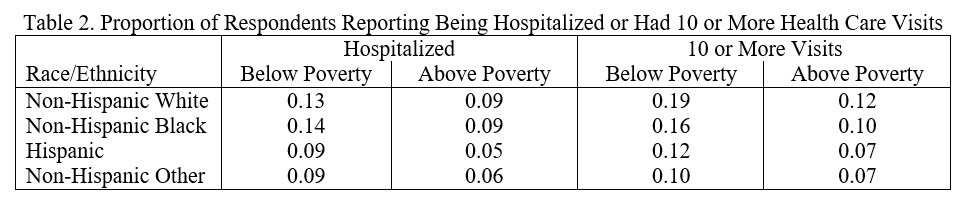
Similar conclusions apply to two different measures of (poor) health: whether a person has been hospitalized in the last year and whether they had 10 or more health care visits (Table 2). Poor persons are much more likely to be hospitalized and to have 10 or more visits than non-poor persons. Here too, within an income group, White and Black persons have similar health, and Hispanic persons and persons of other races (Other) have better health than White or Black persons.
A central thesis of Arcaya and Schnake-Mahl is that residential segregation independently of race and/or income worsens health, such as those outcomes shown in Tables 1 and 2.
“Methodological limitations and some mixed findings aside, many social epidemiologists see residential segregation by race and class as a "fundamental cause" of health disparities because it shapes exposures to critically important health risks and protective factors.” (Arcaya and Schnake-Mahl)
However, if residential segregation is an independent cause of poor health, as suggested by Arcaya and Schnake-Mahl, then we would expect groups that have the highest rates of segregation to be in the worst health. According to a U.S. Census report, Black persons live in the most segregated (and racially isolated) neighborhoods. Hispanic persons are the group with the next highest rate of residential segregation. Despite these high rates of residential segregation for Black and Hispanic persons, their health is either not very different from, or better than, White persons.
Overall, the evidence in Tables 1 and 2 puts the burden on researchers, such as Arcaya and Schnake-Mahl, to provide more substantial evidence that residential segregation is a significant cause of health disparities beyond individual-level factors, such as race and income.
It is also worthwhile to highlight a key phrase in the above quote from Arcaya and Schnake-Mahl:
“Methodological limitations and some mixed findings aside…”. Social scientists cannot put aside these fundamental issues related to causality to reach conclusions. Credible empirical analyses and a consistent set of findings are required before a conclusion such as “segregation by race and class as a "fundamental cause" of health disparities” can be drawn.
The sparseness of credible and consistent evidence linking residential segregation to health is illustrated by several quotes from recent studies:
“The health effects of segregation are relatively consistent, but complex. Isolation segregation is associated with poor pregnancy outcomes and increased mortality for blacks, but several studies report health-protective effects of living in clustered black neighborhoods net of social and economic isolation. The majority of reviewed studies are cross-sectional and use coarse measures of segregation.” (Kramer and Hogue 2009, p. 178)
“Socioeconomic status explains much of the association between neighborhood racial segregation and health outcomes.” (Sudano et al. 2013, p.89)
“In the fully adjusted model … higher Hispanic …but not Black … segregation was associated with higher cause-specific mortality.” (Pruit et al. 2015, p. 1852)
Of course, there are some articles that report evidence supportive of the hypothesis that residential segregation is harmful to health (e.g., Haynaga et al. 2013; Johnson et al. 2016), but the bottom line is that the causal link between residential segregation and health is decidedly uncertain.
One argument put forth by Arcaya and Schnake-Mahl is that residential segregation is a cause of inadequate access to healthcare and poor-quality healthcare. The evidence to substantiate this claim is tenuous and based on cross-sectional analyses that have well-known limitations (e.g., Weinick et al. 2000). I am unaware of any study that has linked changes in residential segregation to changes in access/quality of healthcare for a given person, for example, remaining residents of a transitioning neighborhood. In addition, the link between access (e.g., insurance) and use of care and health remains sparse. For example, results from the Oregon Medicaid Experiment (Finkelstein et al. 2013) and the more dated RAND Health Insurance Experiment (Newhouse 1993) indicated that despite significant increase in the use of health care services associated with having health insurance (or more generous insurance coverage), there was little differences in health between those with and without insurance (or less generous insurance).
A second argument of Arcaya and Schnake-Mahl is that residential segregation gives rise to a segregated healthcare system with low-quality providers serving residents in segregated neighborhoods. However, as shown by researchers from Dartmouth Atlas of Healthcare (e.g., Baicker et al. 2004; Baicker et al. 2005; Goodman et al. 2010), the association between the quality of care (provided to Medicare patients) and racial disparities is not strong.
“Furthermore, there is no consistent pattern of disparities: some areas may have a wide disparity in one treatment but no disparity in another. The problem of differences in quality of care across regions, as opposed to racial disparities in care, should remain the target of policy makers, as reducing quality disparities would play a major role in improving the health care received by all Americans and by minority Americans in particular.” (Baicker et al. 2005, S42)
In sum, the claim that residential segregation (isolation) is an important cause of health disparities net of individual level factors, such as race and income, is not strong. That does not mean it is not true. There are plausible mechanisms linking residential segregation to health that support the scientific plausibility of the argument (Williams and Cohen 2001). And it is possible (likely) that residential segregation causes poverty and other outcomes that may affect health. However, theory and suggestive and inconsistent empirical evidence is a reason to do more research, but it is not sufficient to make causal claims.




